












































































































Severe obesity can drain health, hope, and bank accounts—but wrestling with insurance rules often feels harder than the surgery itself. In 2025, Kansas regulators will make medically necessary bariatric surgery an essential health benefit on every new individual and small-group policy. Translation: if you live in the Sunflower State, the door to coverage is about to open wider—and we’re going to walk through it together in plain English.
Here’s the game plan we’ll cover:
- Confirm whether your current plan already covers surgery
- Meet the medical criteria insurers demand
- Package a rock-solid pre-authorization request—and appeal if they say no
- Calculate what you’ll still pay out of pocket, plus smart ways to fund it
- Track 2024–25 policy shifts so you don’t leave money on the table
Our goal is simple: turn a paperwork maze into a step-by-step checklist so you can move from I hope to I’m scheduled—without surprise bills.
Understanding the insurance landscape for weight-loss surgery
Why insurers say yes

Picture an insurance executive scrolling through a spreadsheet of long-term claims. Obesity appears everywhere—diabetes, heart disease, sleep apnea, joint replacements—and every line is expensive. Now imagine one procedure that trims many of those future payouts at once. That math, not mercy, is why most major carriers cover bariatric surgery when it is medically necessary.
Studies show gastric bypass and sleeve gastrectomy help patients shed enough weight to reverse or manage costly conditions. Over time, hospital admissions drop, prescription counts shrink, and productivity rises, so the up-front check for surgery often turns into a discount on everything else.
According to an insurance explainer from the Bariatric & Metabolic Center of Colorado, adults living with obesity incur about 81 percent higher healthcare costs than their normal-weight peers.
That number crystallizes why carriers view a one-time surgical payment as cheaper than decades of chronic-disease claims.
Regulators see the same ledger. Medicare approved bariatric procedures years ago, Medicaid programs in more than forty states followed, and private plans raced to stay competitive. Kansas adding surgery to its essential benefits list in 2025 is simply the latest vote of confidence.
The takeaway: insurers already believe the operation saves money; your job is to prove you meet their medical checklist.
Which plans actually pick up the tab?
Employer-sponsored coverage
Large companies compete on benefits and often include bariatric surgery. Smaller firms may buy leaner policies that exclude it. Check your Summary Plan Description or ask HR, “Is bariatric surgery covered on this plan?”
Marketplace (ACA) plans
Coverage depends on each state’s essential health benefits. Kansas will require bariatric coverage on all new and renewing individual or small-group plans starting in 2025, so watch the next open-enrollment window.
Medicare
Covers gastric bypass and sleeve gastrectomy if your BMI is 35 or higher plus at least one obesity-related condition, provided you use a Center of Excellence accredited for bariatrics.
Medicaid
Forty-eight programs, including KanCare, approve surgery when criteria are met. Because not every hospital accepts Medicaid for high-resource operations, call ahead to confirm.
Private individual policies
Non-ACA contracts vary widely. Some mirror marketplace language; others exclude surgery outright. Read the exclusions line by line.
Across every bucket, coverage is binary: either your policy lists bariatric surgery as a covered benefit, or it does not. If it does, the rest of this guide will help you unlock it. If not, plan a switch during the next enrollment period.

Step 1: check your policy
Review your insurance plan
Grab your insurance card, flip it over, and call Member Services. Say, “I need to confirm whether bariatric surgery is a covered benefit on my plan and what requirements I must meet.” Wait for a direct yes or no. Coverage is binary; do not accept “It depends.”
Next, open your benefits booklet—or log into your insurer’s portal—and search for bariatric, obesity treatment, or weight reduction. Look at two sections: Covered services and Exclusions. If surgery appears under Covered services, circle it and note any footnotes about pre-authorization, supervised diets, or BMI thresholds. If it sits under Exclusions, highlight the exact wording; you will need it for appeals or a future plan switch.
Screenshots help. Snap the page that shows coverage (or denial). Those images become evidence if the insurer’s story changes.
Finally, confirm your network. Even a covered surgery is reimbursed at a higher rate only if the hospital and surgeon are in network. Most carriers post searchable provider lists online. Type your bariatric center’s name and verify it shows “in network.” If it does not, ask the center to request a network exception; some payers grant one when no local alternative exists.
Once you know where your plan stands—green light, outright exclusion, or gray area—we can plan next moves. The following section pins down the exact medical criteria you must meet so you can start gathering proof.
Step 2: meet the bariatric surgery requirements
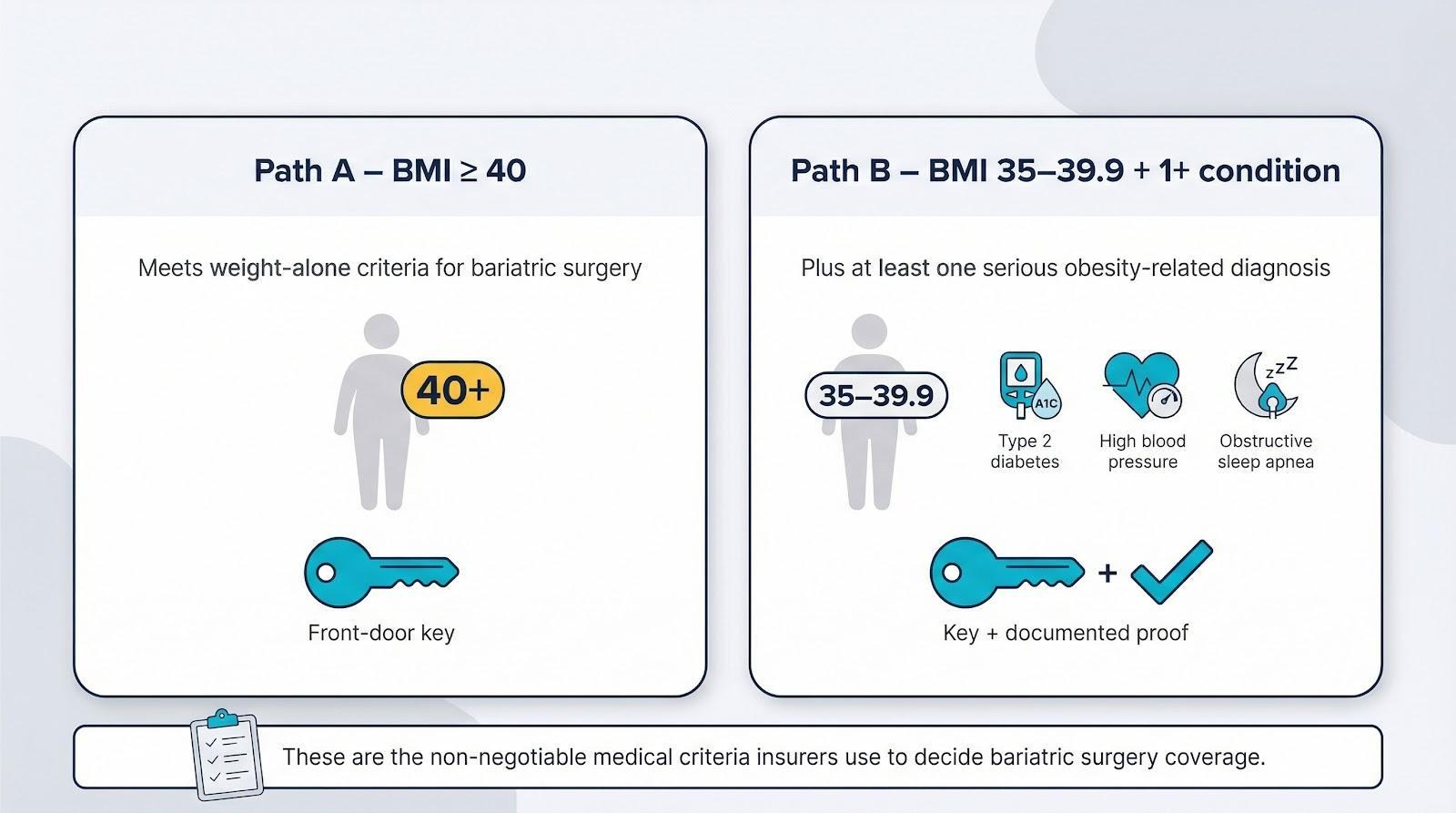
BMI and health conditions: the non-negotiables
Start with the numbers. If your BMI is 40 or higher, you clear the weight-alone bar.
A BMI between 35 and 39.9 must pair with at least one serious obesity-related diagnosis such as type 2 diabetes, high blood pressure, or obstructive sleep apnea.
The bariatric surgery requirements outlined by the Bariatric & Metabolic Center of Colorado also call for a physician-supervised weight-loss program—generally six consecutive months—and spell out procedure-specific rules like avoiding severe GERD before a gastric sleeve.
Treat that external checklist as your audit list while you pull together records.
Think of BMI as the front-door key and your comorbidities as extra proof you belong inside. Make sure those conditions are fully documented: lab results, prescription lists, and sleep-study summaries all help. Before tackling diet logs or psychology clearances, lock down these basics; reviewers cannot waive them.
The paper trail of past attempts
Insurers want evidence that surgery is the last resort, not your first move. Most require a physician-supervised diet program that lasts six consecutive months. Each visit note should record your weight, the counseling provided, and specific behavior goals. Miss a month and the clock restarts, so set reminders.
If you have tried structured programs—WeightWatchers, a GLP-1 medication trial, or hospital meal replacements—gather receipts, progress notes, and weigh-ins. Bundle them chronologically; a thick file speeds approval.
Schedule two clearances early: a psychological evaluation and a nutrition consultation. The psychologist checks for untreated depression, binge-eating, or substance use that could hinder success. The dietitian maps your post-op eating plan so the insurer knows you understand lifelong changes ahead. Most bariatric centers have both specialists in-house.
Nicotine can derail everything. Many carriers require a negative cotinine test for at least 30 to 90 days before surgery. If you smoke or vape, quit now and ask your primary doctor to document each smoke-free visit. A single positive lab result has canceled more surgeries than any BMI dispute.
With BMI, comorbidities, supervised diet notes, psych and nutrition letters, and nicotine-free status in place, you have built a strong case for medical necessity. Next, you will turn that evidence into a pre-authorization packet insurers rarely refuse.
Step 3: prepare your insurance submission
Gather your documentation
Think of the pre-authorization packet as your case file in a courtroom drama. Every exhibit must be numbered, legible, and placed in the exact order the judge—your claims reviewer—expects.
- Letter of medical necessity
Ask your primary physician to list your height, weight history, BMI, and each obesity-related diagnosis, then add a clear statement: “Bariatric surgery is medically necessary to prevent further deterioration of the patient’s health.” Request the letter on practice letterhead, signed in blue ink. - Six months of supervised diet notes
Staple the notes chronologically so weight trends are obvious. If you used a structured program instead, include attendance logs, meal plans, and weigh-ins. - Psychology and nutrition clearances
These letters confirm you understand the lifestyle changes ahead and have no untreated conditions that might hinder success. - Nicotine-test result
Place the negative cotinine report immediately after the clearance letters. - Lab reports and specialist letters
Include any imaging or test results that prove comorbidities. Bold or underline abnormal values to highlight the cost of inaction.
When the stack feels complete, scan it into one PDF. Add bookmarks for each section so reviewers can jump straight to what matters. A tidy, page-numbered file signals professionalism and speeds approval.
Step 4: what to expect on decision day
If you are approved
The call or letter arrives: “Your bariatric surgery has been authorized.” Exhale, then read the fine print twice. Approval letters list the procedure authorized, an authorization code, and an expiration date—usually 90 to 180 days. Mark that deadline on your calendar; surgery must happen before it or you start over.
Next, phone your surgeon’s scheduler. Operating rooms fill quickly, so reserve a date that leaves enough time for any remaining lab work or pre-op classes. Ask for an estimate of your financial responsibility based on the insurance breakdown. Knowing the figure upfront lets you arrange a payment plan instead of scrambling later.
Keep every approval page in a safe, shareable spot—cloud folder and printed copy—because hospitals, anesthesiologists, and equipment vendors will each ask for proof. Showing that single sheet reminds every downstream biller that the insurer already agreed to pay.
If you are denied
Denial letters sting, but treat them as a playbook, not a verdict. The first page lists the exact reason your request failed: missing diet documentation, BMI recorded at 39 instead of 40, policy exclusion language, or “not medically necessary.” Highlight that sentence; everything you do next addresses those words directly.
Call your surgeon’s insurance coordinator that day. Ask whether the office can request a peer-to-peer review, a brief call where your surgeon explains the facts to the insurer’s doctor. Many denials flip when a physician clarifies a misunderstood note.
While the call is in motion, draft a written appeal. Open with your policy number and the denial code, then rebut point by point. Attach the missing diet logs, the sleep-study report showing severe apnea, or the page of your plan that promises coverage. Keep the tone factual and professional; anger muddies strong evidence.

Upload or mail the appeal before the deadline printed in the letter—usually 30 or 60 days. Miss that window and you wait until the next plan year.
If the insurer upholds its decision, escalate to a second-level appeal or request an external review through the Kansas Department of Insurance. Independent reviewers are paid by the state, not the insurer, and their rulings are binding.

Kansas Department of Insurance complaint and external review page screenshot
Persistence pays. Many patients win on the second or third round because each submission closes another paperwork gap. Until you exhaust every appeal tier, “no” simply means “not yet.”
Step 5: financial realities – what insurance covers and what you pay
Insurance coverage breakdown
Approval is not a blank check. Insurers pay only for services coded as part of the operation and only at the contracted rate for in-network providers.
Hospital charges—operating room, recovery bed, nursing care—hit the insurer first. The carrier reimburses the hospital according to a negotiated fee schedule. Your surgeon, anesthesiologist, and any assisting physicians bill separately; their claims follow the same rules. As long as every professional is in network and the CPT code matches the procedure authorized, the insurer pays its share without fuss.
Pre-operative tests ordered within thirty days—blood work, EKG, chest X-ray—count as part of the surgical episode. Post-op visits during the global period, usually ninety days, are bundled, so you will not owe a copay for routine follow-ups.
Coverage stops at anything labeled optional or ancillary. Protein shakes for your liquid phase, lifelong vitamin packs, and future body-contouring surgery fall outside approved codes, so those bills land with you.
Your out-of-pocket costs
Numbers beat percentages, so plug in a realistic Kansas scenario. Suppose your gastric sleeve bills at $20,000 and your plan carries a $2,000 deductible, 20 percent coinsurance, and a $6,000 out-of-pocket maximum.

- You pay the first $2,000 to meet the deductible.
- The remaining $18,000 is split: insurer covers 80 percent ($14,400) and you cover 20 percent ($3,600).
- Add the two figures: your cost is $5,600, still below the $6,000 cap, so any follow-up care that year is essentially free.
If you have already met part of your deductible, the math improves. A high-deductible plan can push your share higher, sometimes past $8,000, before the out-of-pocket ceiling applies.
Plan ahead by setting aside money in an HSA or FSA if available. Those dollars go in tax-free and come out tax-free for qualified medical expenses, turning a $5,600 bill into roughly $4,300 after taxes for many households.
Before surgery, ask the hospital’s billing office for a no-interest payment plan. Most facilities will spread your balance over six to eighteen months, making the cost feel like a car payment instead of a crisis.
Knowing these figures upfront keeps sticker shock off your recovery checklist. Next, we will look at policy trends that could trim costs even further.
Step 6: trends and changes in bariatric coverage (2024–25)
Policy shifts you should watch
Bariatric coverage sits at the center of several fast-moving reforms. The headline for Kansans is the 2025 essential-benefit upgrade: every new or renewing individual and small-group policy must include medically necessary weight-loss surgery, turning what was once a plan-by-plan perk into a statewide guarantee.
Neighboring states preview how momentum spreads. Colorado’s marketplace added bariatric surgery to its standard benefits in 2023, and Minnesota lawmakers are debating a bill that bundles surgery, nutrition counseling, and GLP-1 medications into one obesity-treatment mandate. As more states adopt similar rules, insurers operating across state lines often streamline benefits everywhere instead of maintaining patchwork exclusions.

National guidelines are loosening as well. The American Society for Metabolic and Bariatric Surgery now recommends surgery for some patients with a BMI of 30–34.9 plus type 2 diabetes, a change that pressures insurers to broaden eligibility. A 2024 Northwestern University study found that surgery delivers more health benefit per dollar than long-term GLP-1 drug therapy; actuaries pay attention to that math, and policies usually follow.
For you, these changes translate to leverage. If your plan still drags its feet, point to Kansas’s new rule, neighboring precedents, and evolving clinical standards in your next appeal. Insurers read the same headlines you do, and reminding them of the political and economic tide can nudge borderline cases into the approval column.
Conclusion & key takeaways
You have walked the full insurance gauntlet, from checking the fine print on your card to appealing a denial and budgeting every dollar for surgery day. At each step, the pattern stays the same: document thoroughly, ask directly, and push back when an answer feels vague or unfair.
Post these three truths on your fridge:
- Coverage hinges on proof, not persuasion. Meet the BMI-plus-comorbidity rules, show six months of supervised effort, and hand insurers a packet so complete they approve it on the first pass.
- Kansas tilts the odds in your favor. Beginning in 2025, state law makes weight-loss surgery an essential health benefit for individual and small-group plans. Use that leverage in every call, appeal, and open-enrollment choice.
- Out-of-pocket costs are predictable, and manageable. Know your deductible, coinsurance, and out-of-pocket max before the first incision, then pair them with HSA dollars or a hospital payment plan. The final bill rarely derails the bigger goal: a longer, healthier life.
Bariatric surgery is not a shortcut; it is a serious medical tool. Now you have the map, compass, and local insight to secure coverage. Make the call, gather the records, and step onto the path thousands have taken from doubt to done.



